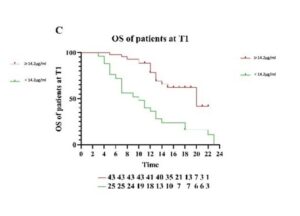
A recent clincial trial compared immunotherapy response in lung and digestive tract cancers to patients levels of zinc. Not only was zinc identifed as an independent indicator of likely positive response to therapy, but also a major factor in reducing progression risks. This is similar results with sodium though with a lower impact level. More data like this is emerging for magnesium.
Zinc deficiency has a role in cancer formation and progression, most studied in prostate cancers but also seen in tissue samples of kidney, liver, ovarian, cervical, pancreas. esophageal cancers. Very recent meta-analysis into breast cancer survival over 10 years showed that higher pre-diagnosis levels were associated with better outcomes, whilst higher copper levels reduced survival (see Concerns). The research discusses low dose zinc supplementation, while other researcher suggest active treatment with copper chelation . Curcumin is known as a natural copper chelator [absorber].
Similar research has shown increased survival benefits for relatively higher selenium-zinc combined levels – including liver, lung, kidney and throat cancer. And in immunotherapy responses, up to 50% of tumors show low expression of so called CDKN2A activity resulting in high metabolic demand for zinc in the tumor microenvironment. This weakens natural immune response to cancer. In pre-clinical study, zinc supplementation was able to reverse this.
Zinc contributes to healthy cell proliferation, differentiation, and mortality (via apoptosis). Zinc levels have been shown in meta-analysis to play a clear and significant role in moderation of insulin resistance and systemic inflammation levels (see References), both of which are linked to faster cancer progression rates. Its important to raise levels before and during treatment based on the clinical observations in outcomes.
Clinical trials during therapy remain few in number. A recent 2023 publication in US does show benefits for prostate cancer risks for progression with a strong association to low dose zinc 1- 24 mg daily (see references). However, this was indicated for patients who took these supplements both before and after diagnosis, whilst significant effects were not reported for use only during a treatment phase.
Doses >75 or 100mg daily is reported as a risk factor for breast and prostate cancer including metastasis. The consensus then, is that low dose zinc 15 to 20 mg or so and in conjunction with low dose dietary selenium, shows clear advantages in both prevention and slowing of disease for some cancers. Levels that can come from dietary sources in the first instance. Where dietary source may be lacking, supplements are a complementary solution, if following a largely vegan/ vegetarian regime for instance.